
56 Sleep and EEG
Sleep is such an important part of our lives that a lack of it strongly correlates with negative outcomes on nearly every measure of health. People who sleep less than approximately 7 hours a night are at a greater risk for heart disease, stroke, asthma, arthritis, depression, and diabetes. Nearly 20% of all car crashes, both fatal and nonfatal, are attributed to drowsy driving. The cancer research branch of the World Health Organization has determined that disruption of regular sleep is “probably carcinogenic to humans”, putting it in the same risk category as the infectious agents malaria and human papillomavirus (HPV), as well as the biochemical weapon mustard gas. Sexual health is affected by sleep deprivation as well, as men with the worst sleeping habits have significantly lower sperm counts, decreased circulating testosterone, and even testicular shrinkage.
Despite all that we know about the benefits of sleep, sleep is often the first time commitment to get cut, often getting squeezed as people stay awake later while waking up sooner. Consider that the CDC estimates that more than a third of American adults fail to get enough sleep each night. Almost 70% of college students fail to get the recommended amount of nightly sleep, and half of all college students report experiencing daytime sleepiness as a result.
The current medical recommendation is 7-9 hours of sleep each night. But why is sleep so important? It is possible to study sleep using a combination of techniques; the output of sleep studies are visualized on a polysomnogram (pahle-SOM-nuh-gram; somn- is the prefix referring to sleep). Several physiological measures are taken in a polysomnogram, including heart rate, blood pressure and oxygenation level, respiratory depth and pattern, muscle activity, eye movement, and one of major interest to neuroscientists: brain wave activity. While everyone knows what sleep is, it is useful to try to more precisely define sleep as a biological function.
Sleep is characterized by a decrease in physical activity, a decoupling from external inputs, and changes in brain wave activity.
Compared to waking behavior, a person’s physical activity is greatly decreased when they sleep. While asleep, people are relatively inactive and as a result, the body uses about 10% less energy. This is not to say that people do not completely cease all movement during sleep. It is very common to readjust posture many times in the middle of the night. Some people may grind their teeth together or talk in their sleep, sometimes carrying on full conversations by themselves! About 15% of people have experienced somnambulism, or sleepwalking: full on wake-like behaviors, such as navigating down a flight of stairs or preparing a sandwich, performed entirely in the absence of intent of memory recall. Despite these rare occurrences of physical activity, the average movement of the person over a night’s rest is still less than their average activity when awake.
When we sleep, our conscious brains are “distanced” from the outside world. Sleep causes a heightened threshold for detection of stimuli, so we do not receive the same magnitude of inputs from our sensory systems as when we’re awake. This is why someone else might have to talk loudly or even shake you physically to wake you up.
Lastly, sleep was once thought to be a period of time characterized by low brain activity. After all, the person looks like they are not moving. Shouldn’t brain activity be reflective of that decreased state of activity? With the advancement of EEG technology in 1924, and the rise of sleep laboratories in the 1970s, scientists who studied brain activity noticed that, at different times throughout the night, the brain of a sleeping person was very similar in activity to the brain of an awake person!
EEG
Electroencephalography (EEG) is used to measure brain rhythms through recording electrical activity at the scalp, making it a non-invasive and painless tool to detect brain activity. EEG detects the general activity of the cortex by measuring small (~10 uV) fluctuations in voltage. This technique does not measure electrical activity of a single neuron, but rather measures the electrical activity of a large population of neurons, on the order of thousands of cells, in order to generate a signal that is large enough to detect.
An EEG reading depicts differences in both amplitude and frequency over time. An increase in amplitude on an EEG indicates a higher degree of synchronous activity of cortical neurons, whereas the frequency of an EEG indicates how often neural synchrony occurs. EEG is used to measure patterns of brain activity during different behavioral states and is used in both research and in the diagnosis of various neurological conditions such as sleep disorders and epilepsy.
How is synchronous activity generated?
Though EEG is used to measure brain rhythms, the function of these rhythms is unknown, but they have been correlated to different behavioral states such as wakefulness, sleep, attentiveness, and various pathologies. Brain rhythms generated through synchronous neuron activity can be created through two different mechanisms.
- Cells within the thalamus have been demonstrated to have pacemaker properties that allow it to generate rhythmical cortical activity.
- Collections of cells can also generate intrinsic rhythms through their collective activity.
EEG patterns during sleep
Each night when we go to sleep, our brains undergo a very stereotyped pattern of activity changes. At times, neurons in the cortex exhibit synchronized patterns of firing. And at other times, cortical activity looks very similar to an awake brain. We can divide sleep roughly into two different phases depending on one of the first physiological measures that sleep scientists studied: eye movement. A study published in 1953 used a device to detect eye movement while a person was asleep. Interestingly, they noticed that at some points in the night, usually first occurring around three hours after falling asleep, the patient’s eyes would dart rapidly and jerkily back and forth, a pattern of activity that the University of Chicago researchers called rapid eye movement (REM). This first period of REM activity lasted for about 20 minutes, after which the eyes would stop moving again. This activity pattern repeated every hour or two for the rest of the night. They used eye movement to separate sleep into two phases: REM sleep, and nonREM sleep (NREM sleep).
In addition to eye movement, they observed and measured other physiological behaviors. Respiration rate and heart rate both increased during the REM phase of sleep and dipped during NREM sleep. They also (rudely) woke up patients throughout the two phases of sleep and found that patients were more likely to recall dreams with visual imagery if their REM sleep was interrupted. Those woken during NREM sleep were less likely to recall dreams, hinting that dreaming is more likely to happen during REM sleep. While eye movement could differentiate between two phases of sleep, EEG could further subdivide NREM sleep. Using EEG, scientists discovered three distinct NREM phases based on neuron activity patterns: NREM1, NREM2, and NREM3 sleep.
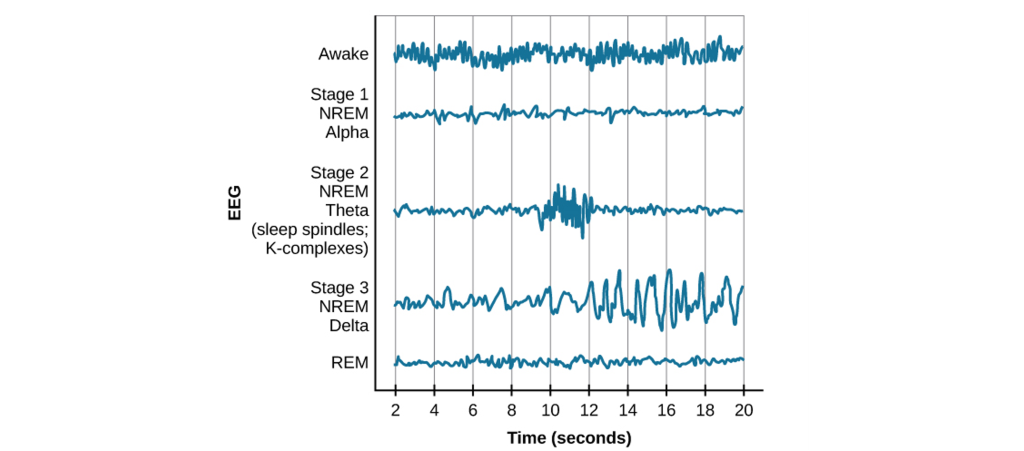
Currently, readings collected via EEG are considered to be the gold standard for measuring the stages of sleep. But before we describe EEG traces while asleep, we should describe the EEG of a person who is awake. Usually, the awake EEG is dominated by high-frequency waves that increase with attention and mental activity.
NREM1 is the earliest stage of sleep. It’s also described as relaxed wakefulness, drowsiness, or light sleep. During NREM1, mostly alpha waves are present and a person’s muscles are still somewhat active. Their eyelids may open and close every so often, and they may still respond to questions. Basically, the deeper into NREM1 sleep a person becomes, more waves with lower and lower frequencies start to emerge. NREM1 transitions into NREM2, which mostly has theta waves.
Lastly, NREM3 occurs, which is also called deep sleep. At this phase of the night, a person’s physiological activity drops to its lowest point of the night: heart rate, respiration, blood pressure, and metabolism all reach minimum during NREM3. In this stage of sleep, many of the cortical neurons fire in synchronicity with one another, and the subsequent change in potentials cause large amplitude deflections in the EEG, called delta waves.
The EEG trace of a person in REM sleep is quite the opposite of what is seen in deep sleep. Instead of large amplitude events at a low frequency, the REM brain has a lot of low amplitude events at a high frequency. In fact, the brain in REM sleep has a pattern of activity that is more similar to a person who is awake than asleep! Because of this asynchronous firing activity, REM sleep is sometimes also called paradoxical sleep.
Progression through the stages of sleep
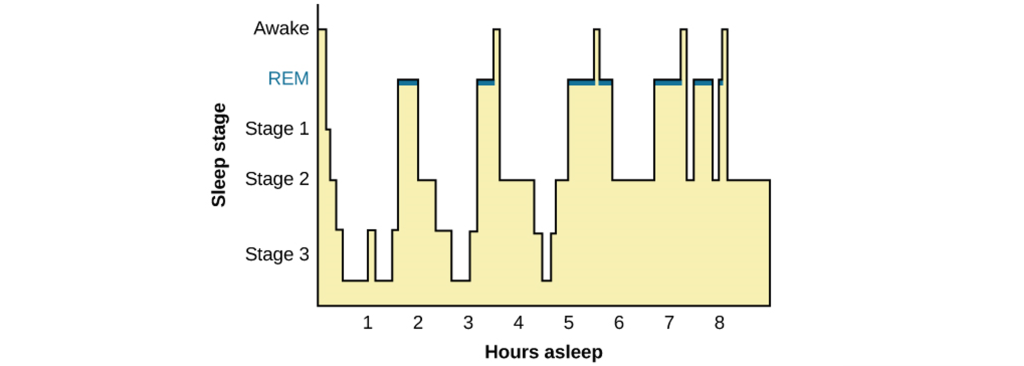
To illustrate the stages of sleep that a person experiences each night, we can use a hypnogram. These charts plot time on the x-axis and stage of sleep on the y-axis. Awake is represented at the top, and deep sleep is at the bottom. For an average night’s rest, neural activity will fluctuate through the four phases relatively predictably. When a person first falls asleep, they will move from NREM1 down through NREM2 then NREM3, before coming back out of deep sleep progressively back to NREM1. After NREM1, they may enter REM sleep before transitioning back through the stages to NREM3 again. This cycle of activity repeats roughly every one and a half hours. People spend a larger percentage of each cycle in deep sleep and very little time in REM sleep early in the night. On the other hand, in the last few cycles before waking up from a full night’s rest, people spend a larger percentage of each cycle in REM sleep, and almost no time in deep sleep.
Why do we sleep?
All organisms that we know of experience some type of sleep. But we still haven’t figured out exactly why animals sleep. Here, we will discuss three theories that have been proposed to explain sleep. None of these theories alone fully explains the complex phenomenon of sleep, and they are not mutually exclusive. The most likely reason we sleep is probably some combination of the following three theories.
Recuperation Theory
The recuperation theory of sleep is centered around the idea that being awake is stressful and exerts a physically demanding toll on the body. The body therefore needs a period of time when energy usage decreases and the body’s natural repair systems can work without disruption. Sleep is how the body “wipes the slate clean” and resets. Evidence for the recuperation theory comes from experiments tailored around the idea of looking at what happens when a person doesn’t get sufficient sleep.
As anyone who has ever pulled an all-nighter can attest, a single night of sleep deprivation often leads to significant psychological changes, including anxiety, irritability, and mood swings. Staying awake even longer than 24 hours can cause more severe changes in mind state, such as temporary psychosis, hallucinations, or delusions.
While the support for the recuperation theory is generally true for almost all people, there are about 1% of people who seemingly gain the restorative benefits of sleep, even with fewer than 6 hours of sleep each night. They may wake up at 4:30 in the morning feeling completely refreshed. And yet, despite getting so little sleep, these short sleepers have similar health outcomes with respect to body mass index and psychiatric measures such as depression and overall optimism. Something about the circadian rhythms of these short sleepers allows them to “maximize” their sleep efficiency. Many have very short sleep latencies, meaning they fall asleep within minutes after lying down—as quickly as someone with narcolepsy. They also spend a larger percentage of their night in deep sleep and REM sleep while minimizing NREM1 and NREM2.
Evolutionary Adaptation Theory
The evolutionary adaptation theory is the idea that animal sleep patterns are different across species for reasons that most efficiently benefit each animal. Over millions of years of evolution, individuals with the most ideal sleep patterns have an advantage, and their sleep habits will be selected for in the following generation. For example, consider humans. As an animal highly dependent on light and the visual system for navigation and accurate performance of tasks, the dark is a very dangerous time to be active. The risks of wandering off a cliff, running head-first into a tree while escaping a predator, or eating a wrong-colored poisonous berry would all be elevated in the dark. We benefit from behaviors that minimize those risks, such as inactivity until the sun rises. During this inactive period, sleeping decreases our metabolism and our body’s need for energy.
Humans are just one animal that has an evolutionarily fine-tuned sleep pattern. If you look across the animal kingdom, you’ll find all varieties of sleep behaviors that are best fitted to the needs of the individual species. In the wild, for example, dolphins are generally prey. They evolved with the ability to put one half of their brain to “sleep” at a time, allowing the “awake” half to keep an eye out for potential predators. Small prey animals, like squirrels, are faced with the threat of being attacked at night. For them, remaining very still, quiet, and hidden improves their survival. Tigers, the top alpha predators in any ecological niche, have almost no predators to hide from, allowing them the luxury of sleeping up to 20 hours a day.
This evolutionary adaptation theory argument has a major weakness, however. In almost all animals, sleep represents a period of time when an organism’s ability to use their sensory organs to detect the hallmark signs of an approaching predator, like the flurry of feathers from a hungry owl or the soft padding of a wolf footsteps, decreases drastically. For an animal that can’t hide very effectively, sleep represents a period of vulnerability, as they would be unable to sense incoming threats.
Brain Plasticity Theory
The brain plasticity theory suggests that the brain needs some period of time for critical changes to occur. During sleep, circuits in the brain undergo consolidation processes that are important for memory formation. For example, academic performance and examination grades worsen as a person’s nightly sleep decreases. Both the REM and NREM3 phases of sleep are important for different types of memories and studies suggest that declarative memory, pieces of information about facts, benefits more from slow-wave sleep while procedural memory, the learning of motor skills, is enhanced by REM sleep.
Although the exact mechanisms about how sleep improves memory are unknown, we theorize that brain activity during sleep helps move memories held in “temporary” areas into areas of stable, long-term storage. The evidence in support of this theory starts with looking at the brains of newborns. When you were first born, during those first few weeks of life, you slept close to nearly 70% of the day, almost 17 hours! At this point in your life, your brain starts to experience all sorts of new sensations: your eyes detect visible light for the first time, the skin feels the air blow past it, and the ears sense new frequencies and combinations of sound waves. As a result of these stimuli, scientists hypothesize that your brain undergoes as many learning events as rapidly as possible. This rapid learning helps you remember what you learned each day so you can respond to your environment as you grow up.
Sleep Disorders
Insomnia
Almost everyone has experienced difficulty sleeping at some point in their lives, often as a result of stress or anxiety. For example, it might be difficult to fall asleep the night before a big interview, or you may wake periodically in the hours before an important early morning flight. There is no strict definition for insomnia. The major clinical symptoms are self-reported measures, such as a dissatisfaction with nightly sleep or a change in daytime behavior, such as sleepiness, difficulty concentrating, or altered mood states. The lack of clear diagnostic criteria makes estimating prevalence difficult, but some guesses put the number of people with insomnia close to one third of the US population. Common triggers for insomnia include heightened anxiety, stress, or advanced age. It may also be downstream of other diseases, such as Parkinson’s disease, diabetes, depression, or chronic pain conditions. Lifestyle can also be a major risk factor for insomnia, as jet lag and working late-night shifts can disrupt sleep patterns.
We can describe insomnia as acting at two stages. Onset insomnia is defined as a difficulty with initially falling asleep. People with onset insomnia will frequently lie in bed for a long time before finally drifting off. Maintenance insomnia, however, is a difficulty with remaining asleep. People with maintenance insomnia experience many waking events throughout the middle of the night, or they may wake up very early in the morning and be unable to get back to sleep. The two are not exclusive, and people may experience both forms of insomnia in a single night.
The most effective treatments for insomnia begin at the level of behavioral changes. Improving sleep habits, such as minimizing arousal states before bedtime, developing a reliable pattern of sleep-wake timing, eliminating caffeine intake in the afternoon and evening, and increasing daytime physical activity can decrease insomnia. Prescription medications are less preferred for insomnia treatment, since these drugs are more effective at inducing unconsciousness rather than biological sleep. These drugs can also have adverse psychological side effects such as mood swings and depression, and those adverse effects may be more severe than insomnia itself. Prolonged use of prescription sleep medications can lead to a “rebound effect”, causing a person to experience even worse insomnia when they are unable to get sleep drugs. This is called iatrogenic insomnia, and can lead to a cycle of dependence.
Narcolepsy
Unlike the previous two sleep disorders, which result in a deficit of sleep, narcolepsy can be thought of as an “excess” of sleep. More accurately, narcolepsy is inappropriate sleep, and it manifests as frequent sleep attacks throughout the day, each event lasting for seconds or minutes at a time. An estimated 1 in 2000 people experience narcolepsy. One of the life-threatening symptoms that appears in narcolepsy is cataplexy, which is the sudden weakening of muscle tone that accompanies a sleep attack. A cataplectic attack may cause someone to physically fall over during a narcoleptic incident. Cataplexy often happens during high emotional states, such as excitement. As with other sleep disorders, changes in lifestyle can improve the course of narcolepsy. Introducing short daily naps can be helpful, as can general good sleep habits (minimal digital device usage before sleep, regular sleep-wake timing, and physical activity). Drugs such as amphetamines (Modafinil) can be used in the daytime to stimulate activity in the CNS and can be prescribed to treat severe cases of narcolepsy. Some antidepressant drugs can be used to treat cataplexy.
The exact cause of narcolepsy has not yet been identified. However, there are many clues that point to a dysregulation of the signaling molecule orexin produced by cells in the lateral hypothalamus. These neurons die off in people with narcolepsy, but the cause of why the neurons die is unknown. Also, having a genetic predisposition to narcolepsy does not guarantee that a person will experience the symptoms, indicating that there is some combination of genetic and environmental factors that lead to narcolepsy.
Fatal familial insomnia
While many cases of sleeplessness last a day or two, and some cases are clinically significant and treatable with behavioral changes, a very small fraction of cases of insomnia are incurable and deadly. In people with fatal familial insomnia (FFI), they experience severe insomnia. Some patients stay awake for up to six months at a time. As a result of either the disease or the sleep deprivation, they experience altered mood states, hallucinations, dementia, and eventually death, usually within two years after a diagnosis is made. The cause of FFI is unknown. There is a strong genetic component associated with it, as it appears frequently within certain family trees. But, there have also been a few cases of sporadic FFI, people with no apparent family members with the disease. One observation in common among people with FFI is significant damage to the thalamus, as a result of misshapen proteins called prions, a similar disease-causing agent that is responsible for mad cow disease.
REM sleep behavior disorder
One very rare sleep disorder called REM sleep behavior disorder (RBD) can cause people to carry out complex, highly coordinated motor actions while they are sleeping, sometimes acting out their dreams as if they were reality. People with RBD are at risk of injuring themselves or others. Their sleep actions may be in response to a violent nightmare, causing them to jump out of bed, kick or punch the air, run through the house, or throw things. One of the most shocking instances of parasomnia-induced sleepwalking was the 1987 case of Kenneth James Parks, a Canadian man who, in his sleep, drove 23 km to the house of his in-laws and stabbed both of them with a kitchen knife. After his arrest, scientists discovered that his brain activity was highly abnormal during sleep. As a result of the medical examination, the Supreme Court of Canada acquitted him of murder in 1992.
Key Takeaways
- EEG is used to measure brain activity through the scalp and is used to measure brain activity during sleep.
- Sleep can be divided into REM and NREM sleep (NREM1, NREM2, NREM3).
- REM sleep EEG readings most closely resemble awake EEG readings.
- The progression of the stages of sleep starts in REM sleep, then progresses through NREM 1, NREM2, and NREM3 before cycling back to REM sleep. As the night progresses, an individual spends more time in REM sleep and less time in deep sleep.
- The reason why we sleep is not fully understood but is likely a combination of three theories: recuperation theory, evolutionary adaption theory, brain plasticity theory.
- There are disorders of sleep that can cause either lack of sleep or excessive sleep.
Attributions
Portions of this chapter were remixed and revised from the following sources:
- Open Neuroscience Initiative by Austin Lim. The original work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
Media Attributions
- EEG recording © Petter Kallioinen adapted by Valerie Hedges is licensed under a CC BY-SA (Attribution ShareAlike) license
- Stages of sleep © Cheryll Fitzpatrick and Christina Thorpe adapted by Valerie Hedges is licensed under a CC BY-SA (Attribution ShareAlike) license
- Progression through stages of sleep © Cheryll Fitzpatrick and Christina Thorpe adapted by Valerie Hedges is licensed under a CC BY-SA (Attribution ShareAlike) license
output of sleep studies
sleepwalking
Noninvasive recording technique used to measure brain activity through the scalp
Height of the action potential (from trough to peak)
rate of activity
Neurological disorder that causes seizures or unusual sensory experiences
A chart that plots time on the x-axis and the stage of sleep on the y-axis. Awake is represented by the top of the chart and deep sleep is at the bottom of the chart
memory that involves remembering events and facts. Also called explicit memory.
Type of unconscious memory that allows for remembering procedures and performance of specific tasks
sudden weakening of muscle tone

{kind=link}