
65 Psychiatric Disorders: Schizophrenia
Schizophrenia is a psychiatric condition affecting just under 1% of people. Schizophrenia affects men slightly more often than women and affects people of all races. There is a strong association between low socioeconomic status and the risk of developing schizophrenia, indicating that stresses such as neonatal nutritional deficiency or food insecurity may be risk factors. Other risk factors that contribute to increased schizophrenia risk include prenatal drug exposure, heavy drug use during early adolescence, and childhood adversity.
A diagnosis is generally made while a person is in their late adolescent years through their thirties. During this phase of life, the brain is still undergoing subtle maturation processes, which may account for why a person is more vulnerable in these years. After this age, the risk of developing schizophrenia decreases significantly. Also, the later in life that schizophrenia symptoms appear, the better the health outcomes are. It is worth noting that people with schizophrenia have the neurotypical range of intelligence, with the occasional outliers: John Nash, the real-life Nobel prize-winning economist depicted in the movie “A Beautiful Mind”, was first diagnosed with schizophrenia in 1959.
Symptoms of Schizophrenia
The symptoms of schizophrenia can be roughly classified into two categories: positive symptoms and negative symptoms. These phrases are used to describe whether there is an excess of some function, (positive symptoms), or a deficit of a function, (negative symptoms). The symptoms do not appear uniformly across patients, so not all patients develop every symptom.
Positive Symptoms
The most well-known positive symptom of schizophrenia is hallucinations, perceiving something that is not there (as opposed to illusions, which are misinterpretations of things that are there). Usually, patients experience auditory hallucinations, but they more rarely have visual hallucinations. The voices that people hear may be consistent or can change over time. Interestingly, the nature of these hallucinations is influenced by society. In cultures with strong ancestor reverence, they may hear the voices of their grandparents, whereas people in religious cultures may hear the voices of deities.
Relatedly, people with schizophrenia may experience a variety of delusions, untrue beliefs that cannot be changed despite overwhelming evidence. The delusions can come and go spontaneously. Delusions exist in many forms. A paranoid delusion is when a person believes that they are being spied on, maybe by the government or by aliens. A persecutory delusion is a persistent thought that the world is out to get them or to do them harm. Delusions of grandeur are when a person has a tremendously high sense of self esteem, believing that they are royalty or are the reincarnation of God.
Other positive symptoms that can present in schizophrenia are a variety of motor disturbances. Basal ganglia and cerebellar structural deficits are found in schizophrenia, two brain structures involved in motor control, which may explain why deficits are observed. One motor difficulty is catatonia, where a person can hold their body in a highly unusual position for a prolonged period of time. They may also display stereotypy, a series of repetitive, purposeless behaviors, such as the persistent rocking of the body or self-caressing.
Negative Symptoms
The negative symptoms of schizophrenia may include deficits in expression. One common symptom is a flat affect, where a patient does not show or express emotion in situations where you would expect to see them. A related negative symptom is alogia, a decrease in the use of language. People with alogia often use vague language that is lacking in content or repetitive. Negative symptoms also include deficits in motivation or interest. Two closely-related negative symptoms include anhedonia, a loss of a sensation of pleasure and the inability to expect upcoming pleasure. Furthermore, patients with schizophrenia may also exhibit avolition, a decrease in goal-directed activity, which can cause a person to stop seeing their friends and cease displaying interest in social gatherings, leading to worsened interpersonal relationships. Negative symptoms may also manifest as a deficit of a patient’s cognitive abilities, particularly shortcomings in episodic memory. They may also present with difficulty in performing attention-related behavioral tasks.
Biological Basis of Schizophrenia
Genetics
Schizophrenia has a strong genetic component, with increased risk associated with having a first-degree relative that has the disease, however most individuals with schizophrenia do not have a family history. Many different genes have been identified in disease onset and progression.
One example supporting the genetic component of schizophrenia are the Genain Quadruplets. They were a set of identical quadruplet sisters that were born in 1930. All four of the sisters developed schizophrenia by the age of 24. The sisters’ paternal grandmother may have had schizophrenia and it was known that they grew up in an abusive household, making it unclear if their development of schizophrenia stemmed from their environment, genetics, or a combination of the two.
Structural Abnormalities in Schizophrenia
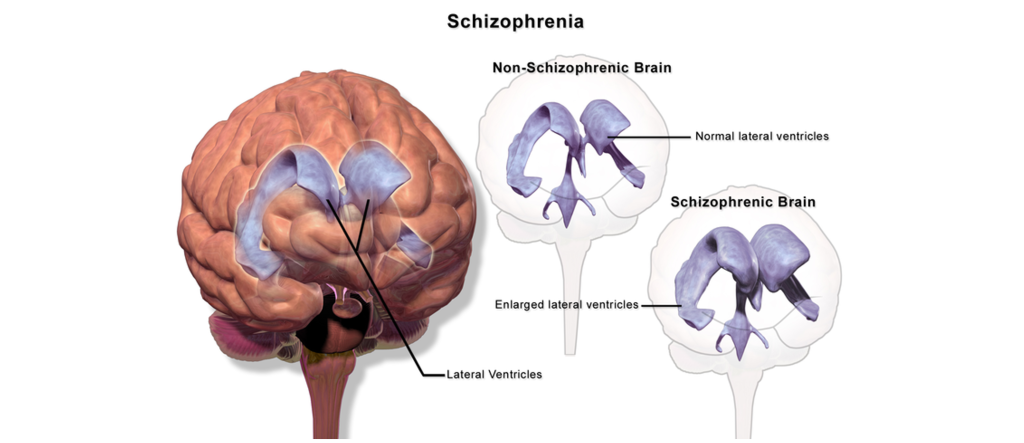
A number of structural abnormalities have been observed in the brains of individuals with schizophrenia. For one, the lateral ventricles are typically enlarged in those with schizophrenia than in those without schizophrenia. The increased size of the lateral ventricles could alter intracerebral pressure or compress the areas of the brain adjacent to the lateral ventricles.
In addition, a decrease in cortical thickness has been observed as well as wider than typical sulci between the gyri. Problems of cell migration during development may also play a part in schizophrenia, leading to abnormal cellular densities and organization. There also seems to be cell loss and disorganized cell location within the prefrontal cortex.
Role of Dopamine in Schizophrenia
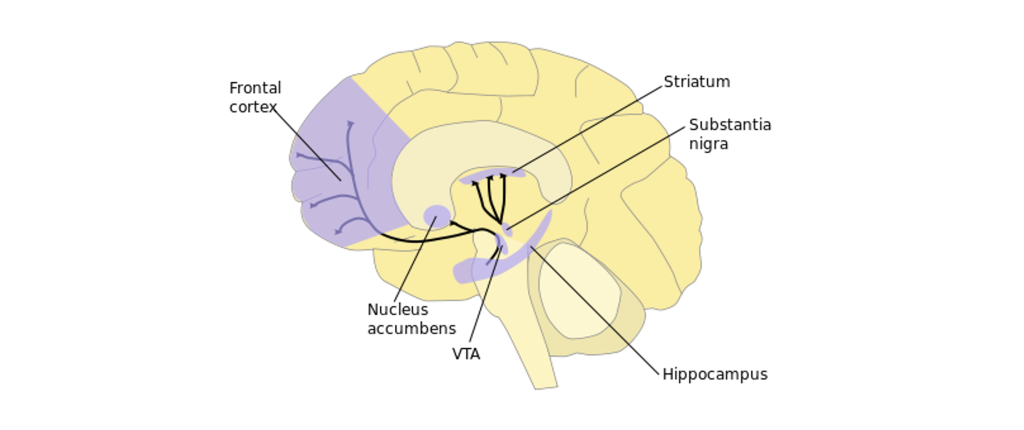
In a healthy person, dopamine is important for motor control and motivation, two behaviors that are changed in patients with schizophrenia. Dopamine receptors (D1 and D2-like receptors) are found throughout the mesolimbic and nigrostriatal dopamine pathways. Therefore, scientists have suggested that increased dopamine signaling may be an underlying root cause in schizophrenia. In fact, psychotic episodes are triggered by activation of dopamine receptors and increased D1 receptor binding has been observed in the prefrontal cortex in those with schizophrenia. While the dopamine hypothesis is one of the earliest theories of schizophrenia, modern genetics studies have shown that polymorphisms in the dopamine D2 receptor are risk factors.
Animal Models of Schizophrenia
One animal model for schizophrenia is based on the hypothesis that excess dopamine leads to the disorder. Introducing high doses of the drug amphetamine, which increases dopaminergic signaling, induces a temporary schizophrenic-like state in non-human animals. The hyperdopaminergic model of schizophrenia produces cognitive deficits with no changes in memory or other negative symptoms. Alternatively, administration of NMDA glutamate receptor antagonists, like ketamine or PCP, is also used as a behavioral model of schizophrenia.
Other non-human models of schizophrenia are neurodevelopmental models. In these models, a pregnant dam is exposed to the compound MAM, which causes the newborns to develop atypically and display behavioral deficits similar to schizophrenia. Inducing an unusually strong immune response in the pregnant mother can also cause atypical development in utero, which causes the animals to experience behavioral deficits after birth. The biggest limiting factor to developing an animal model is that many symptoms in human schizophrenia, like paranoid delusions or auditory hallucinations, are impossible to detect and quantify in nonhumans. The PCP model can cause changes in rodent social behaviors, but it is hard to tell if this model causes any of the positive symptoms that you might see in a patient with schizophrenia. Despite the limitations of these non-human models of schizophrenia, they have been helpful in testing the therapeutic efficacy of anti-schizophrenia drugs.
Treatments for Schizophrenia
Pharmacological Treatments
The dopamine theory of schizophrenia has led to a few novel therapeutic strategies, especially in the context of the dopamine D2 receptor.
Typical, or classical, antipsychotics such as thorazine or haloperidol are more effective treating positive symptoms of schizophrenia such as hallucinations and delusions in some patients. These drugs block D2 dopamine receptors (dopamine antagonists) and decrease dopaminergic signaling, however they have many undesirable motor side effects such as tremors, decreased voluntary movement, tardive dyskinesias, and a shuffling gait named the ‘Thorazine shuffle’. The effectiveness of the antagonist is correlated with the ability of that drug to block the D2 receptor.
Atypical, or nonclassical, antipsychotics such as Clozapine, antagonize a wider array of dopamine receptors in addition to some serotonin and norepinephrine receptors. These drugs more effectively treat negative symptoms of schizophrenia, but also can treat the positive symptoms with less side effects compared to the typical antipsychotics. Unfortunately, pharmacological therapies are not always effective in humans. Around a third of patients discontinue their treatment regimen, and around a fifth of them report adverse side effects such as extrapyramidal motor symptoms, sedation, and weight gain.
Transcranial Magnetic Stimulation
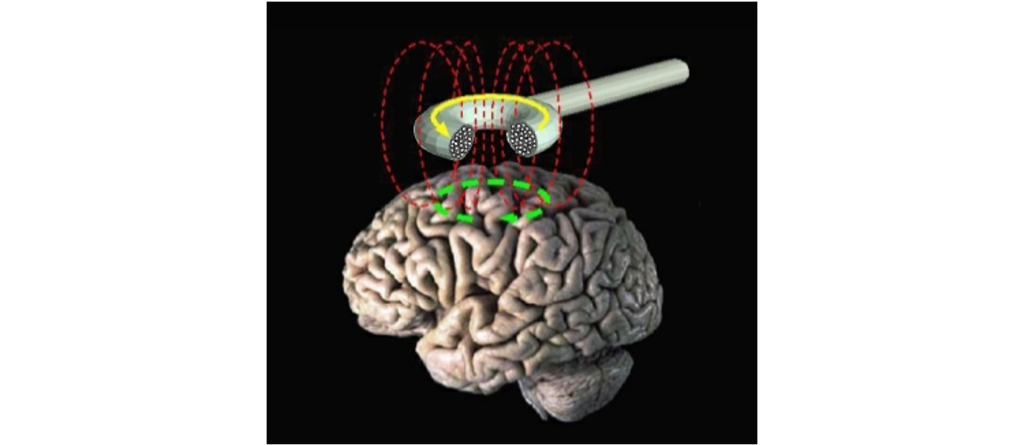
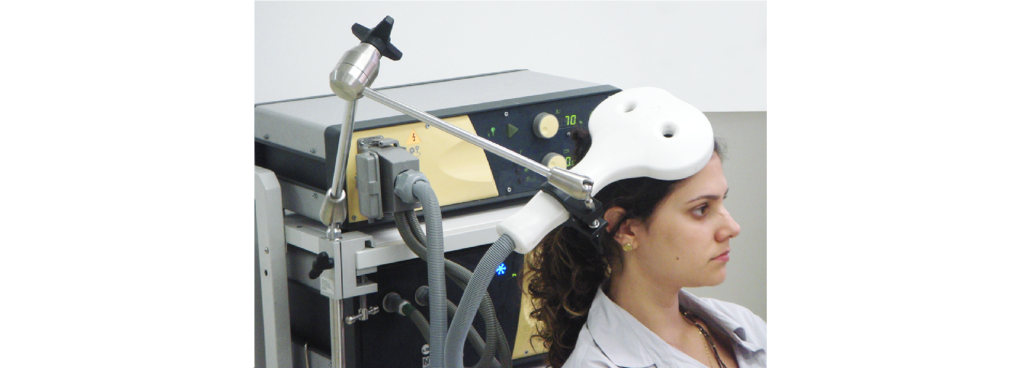
A potential new therapy is based on transcranial magnetic stimulation. In physics, there is a close relationship between electricity and magnetism. The movement of magnets can generate electric currents, and conversely, electricity can generate magnetic fields, a process called induction. A brain stimulation technique called transcranial magnetic stimulation (TMS) relies on induction to generate electrical currents through the skull. The TMS machine itself is a handheld coil of wires in a loop. Passing electrical current through that loop produces a magnetic field. The magnetic field generated then induces an electrical current at some distance away from the coil. By placing the coil at the surface of the scalp, we can electrically activate small areas of brain tissue.
For instance, using TMS above the motor cortex causes muscle contractions, and using TMS above the occipital lobe causes the perception of flashes of light. A single pulse of TMS delivered to the right motor cortex will produces electrical activity in the motor nerve of the left hand, causing it to twitch. In repetitive TMS (rTMS) multiple pulses are delivered, which has been demonstrated to produce long-lasting effects that extend beyond the stimulation period. rTMS can be used to produce either inhibition in brain targets, through low frequency rTMS, or to produce excitation to the brain through high frequency rTMS.
TMS is believed to have moderate benefits for several different psychiatric conditions, potentially making it a meaningful therapeutic intervention. Single pulse TMS can be used to evaluate damage from stroke, ALS, multiple sclerosis, and a number of motor disorders. It has also been approved for the treatment of migraines. rTMS delivered to the motor cortex may help alleviate chronic pain conditions, Parkinsonian symptoms, and improve contralateral motor function following stroke injury. Further, rTMS activation of prefrontal cortex can decrease anxiety, antidepressive symptoms, cigarette craving or consumption, and schizophrenia. Stimulation of other brain regions can be antiepileptic and may also minimize auditory hallucinations or tinnitus (ringing in the ears.) In schizophrenia, some evidence suggests that targeted activation of the cortex can decrease the severity of auditory hallucinations. There may also be some mild improvements in the negative symptoms.
The technique itself is completely noninvasive. TMS can be delivered simply with placement of the electric coil on the surface of the head. TMS may have some unexpected consequences, such as temporary headaches, localized pain, changes in hearing, and bizarre changes in somatosensation. The most severe side effect so far recorded is seizures, which can be very dangerous. Use of TMS is still highly experimental. As with fMRI, the magnetic fields generated by a TMS device can cause dangerous interactions with any magnetosensitive implants, such as deep brain stimulation devices, cochlear implants, or aneurysm clips.
Key Takeaways
- Schizophrenia is a psychiatric condition that has both genetic and environmental components.
- The symptoms of schizophrenia are classified into two categories: positive symptoms (addition of function) or negative symptoms (subtraction of a function).
- A number of structural abnormalities have been observed in schizophrenia.
- There are animal models that help model some of the symptoms of schizophrenia, but modeling hallucinations and delusions is not possible in animal models.
- Excess dopamine signaling has been implicated in schizophrenia and pharmacological treatments are aimed at decreasing dopaminergic signaling.
- Transcranial magnetic stimulation is a newer technique that is being used to treat a number of different psychiatric disorders.
Attributions
Portions of this chapter were remixed and revised from the following sources:
- Open Neuroscience Initiative by Austin Lim. The original work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
Media Attributions
- catatonia © ункноњн adapted by Valerie Hedges is licensed under a Public Domain license
- enlarged ventricles © BruceBlaus adapted by Valerie Hedges is licensed under a CC BY-SA (Attribution ShareAlike) license
- dopamine pathways © NIDA adapted by Valerie Hedges is licensed under a Public Domain license
- TMS © Eric Wassermann, M.D. adapted by Valerie Hedges is licensed under a Public Domain license
- TMS on person © Eric Wassermann, M.D. adapted by Valerie Hedges is licensed under a Public Domain license
addition of a symptom or excess of a symptom
decrease or deficit in a function associated with a symptom
perceiving something that is not there
untrue beliefs that cannot be changed despite overwhelming evidence
a group of symptoms that can include a lack of movement or unusual movement and communication.
repetitive, purposeless behaviors
decreased use of language
loss of pleasure
decrease in goal-related activity

{kind=link}
.png){kind=link}
{kind=link}
{kind=link}