
51 Drug Addiction
In the United States, more than 59 million people aged 12 and over have used illegal drugs or misused prescription drugs within the last year. Use of some of these drugs carry significant health risks, and their use has led to hundreds of thousands of deaths, making drug use one of the highest preventable causes of mortality. For some people, drug use turns into a substance use disorder, or addiction. Importantly, many more individuals misuse drugs than are drug-dependent.
What is drug addiction?
Substance use disorder, typically referred to as addiction has many different facets.
The American Society of Addiction Medicine defines drug addiction as “a primary, chronic disease of brain reward, motivation, memory and related circuitry. Dysfunction in these circuits leads to characteristic biological , psychological, social and spiritual manifestations. This is reflected in an individual pathologically pursuing reward and/or relief by substance use and other behaviors.”
Diagnosis of Substance Use Disorder
One of the major challenges with understanding substance use disorder and other brain disorders is related to the difficulty of making an accurate diagnosis as almost everything in biology exists on a spectrum. To help establish a diagnosis, the American Psychiatric Association (APA) has put together a series of criteria for psychiatrists to diagnose these complex conditions. The guidelines are compiled in a book called the Diagnostic and Statistical Manual of Mental Disorders. They are currently on the fifth revision of the text, referred to as the DSM-5. It’s an imperfect set of criteria, but it is a start towards understanding these remarkably complicated conditions.
According to DSM-5, a substance use disorder may be an appropriate diagnosis when at least two of the following characteristics occur within a 12-month period of time and cause significant impairment or distress:
- The quantity of the substance used or the amount of time spent using is often greater than intended;
- Efforts to control use of the substance are unsuccessful due to a persistent desire for the substance;
- Considerable time is spent using the substance, recovering from its effects, or attempting to obtain the substance;
- A strong desire, craving, or urge to use the substance is present;
- Substance use interferes with major role obligations at work, school, or home;
- Use of the substance continues despite harmful social or interpersonal effects caused or made worse by substance use;
- Participation in social, work, or leisure activities is avoided or reduced due to substance use;
- Substance use occurs in situations where substance use may be physically hazardous;
- Continued substance use occurs even when the substance is causing physical or psychological problems or making these problems worse;
- Tolerance for the substance develops, including a need for increasing quantities of the substance to achieve intoxication or desired effects or a noticeable decrease in effects when using the same amount of the substance;
- After heavy or sustained use of a substance, reduction in or abstinence from the substance results in withdrawal symptoms or precipitates resumption of use of the substance or similar substances to relieve or avoid withdrawal symptoms.
Cost of Substance Use
Substance use disorder is prevalent worldwide. On top of the direct health risks associated with compulsive drug use, drug addiction has a tremendous financial burden: Alcohol, tobacco, and illicit drugs cost the US more than $740 billion dollars in lost productivity, health care costs, and legal related fees and fines.
In the early 1900s, US laws regulating the manufacturing, distribution, possession, and use of drugs were complicated. Certain substances were banned, but regulation of the substances was left largely to individual states. It wasn’t until 1970 when a nationwide proposed regulatory measure would combine all of the current federal mandates regarding misused drugs into a single bill, and Richard Nixon signed the Controlled Substances Act (CSA) into law. Under the terms of the CSA, the Drug Enforcement Agency and the Food and Drug Administration would be responsible for developing regulations about a wide variety of chemical substances. For each drug, they would be tasked with evaluating the health-related properties of the drug and its impact on health, including toxicity, harm, and addiction potential.
Despite a dramatic increase in the cost of drug enforcement that followed the signing of the Controlled Substances Act, the rate of drug addiction in the United States has remained unchanged.
Abused Substances
Drugs are defined as chemical substances that come from outside the body; drugs are exogenous substances that can influence a person’s physical or mental state. Keeping in mind the impact on health and addiction potential, drugs are classified into one of five categories, rated Schedule I through Schedule V.
Drugs put into Schedule I are substances that were perceived to have the highest addiction potential, most severe health risks, and no medical applications. On the other end of the spectrum are Schedule V substances, drugs with low addiction potential, few health risks, and legitimate uses within the clinical setting. Substances classified under Schedule I include heroin, for example, while a Schedule V substance might be an antiepileptic drug like Lyrica. Today, the list of controlled substances contains more than 400 chemicals. Interesting, neither tobacco or alcohol is regulated under the terms of the Controlled Substances Act, despite these drugs being among the most misused in the US with tremendous health risks, high addiction potential, and little medical application. There are probably thousands and thousands of psychoactive substances, chemicals that can act on the nervous system which can induce a change in behavior or mind state.
Some major abused drugs are described below.
Alcohol
According to the 2015 National Survey on Drug Use and Health, alcohol is the most widely used substance among these drugs, with more than 85% of adults reporting having used alcohol at some point in their lives. Chemically speaking, many substances are classified as “alcohols”, but the most common misused is ethyl alcohol or ethanol. Ethanol is an easily-obtained substance with a highly intoxicating effect. The overwhelming majority of ethanol use is recreational. The World Health Organization reports that alcohol use is the leading risk factor for premature death among males aged 15-59 globally, making it one of the overall top causes of preventable death. Acute exposure to ethanol has effects that differ depending on dosage.
At low concentrations, ethanol can induce an elevation in mood, decreased anxiety, increased risk taking, slowing of reflexes, and impaired judgment. At high concentrations, ethanol can cause memory deficits, loss of consciousness, analgesia and areflexia, and possible death through respiratory depression. Chronic exposure to low levels of alcohol has some pro-health benefits such as decreased risk of death by cardiovascular events, but in general, these benefits are outweighed by negative health outcomes.
Nicotine
Nicotine is the main psychoactive ingredient of tobacco products. Nicotine is an alkaloid compound that is synthesized in nature by a variety of plants, with the tobacco plant having the highest nicotine content. Other plants of the Solanaceae family (Nightshade family), such as eggplants and tomatoes, also contains nicotine, as it was probably an anti-herbivory evolutionary adaptation. The most common routes of administration for nicotine include inhalation (cigarettes, cigars, vape), transbuccal (chew, dip, snuff), or transdermal (in the case of the nicotine replacement therapeutic strategy: the nicotine patch). Nicotine is a highly addictive substance, often rated as addictive as cocaine or heroin. It is currently the leading cause of preventable death in the US, causing nearly one out of every five deaths.
When a person smokes a cigarette, they experience a rapid rush or a high within tens of seconds. Chronic smoking greatly increases the risk of developing lung, throat, and mouth cancers, coronary heart disease, or stroke. Cigarette smoking over the past several decades has seen a sharp decline, in part due to the success of anti-smoking campaigns in changing public opinion toward smoking, and government-led changes in legislation resulting in stricter marketing laws, especially in regards to targeted advertising aimed at youth. In the mid 1970’s, almost 30% of 12th graders reported smoking cigarettes daily, and that number has decreased to only 4% in 2018. On the other hand, the rising popularity of vape among teenagers has encouraged nicotine consumption through an alternate route of administration: Teen e-cigarette users are more than 3 times more likely to start smoking cigarettes compared to non e-cigarette users.
Cannabis
Cannabis is a drug that is derived from the flowering buds or other parts of the Cannabis sativa plant. The most common route of administration is inhalation, or smoking. As cannabis becomes decriminalized or outright legalized across the US, oral preparations are becoming more commonplace. The effects of cannabis are often felt within minutes, and can include a sense of euphoria, relaxation, distortion in the sense of perception, and potentially a lightness (high) or a heaviness of body (stoned). Cannabis is currently classified as a Schedule I drug federally, but as of 2022, 23 states/territories have legalized recreational use of cannabis, and only 12 states do not permit cannabis for medicinal use.
The stigma surrounding the “evils” of cannabis use are largely a remnant of a morality propaganda campaign driven by the publishing of such “educational” films as Reefer Madness in 1936. Much of our current medical understanding of cannabis is that it is far less harmful than once believed, although it does have a negative impact on the developing brain, as significant adolescent exposure to cannabis increases the likelihood of developing psychiatric conditions such as schizophrenia later in life.
Opioids
Opioids are a class of drugs, either natural or synthetic, that can bind to and activate the body’s endogenous complement of opioid receptors. The most well known natural opioid is opium, but the other popular drugs of this class include the street drug heroin or the medicinal substances morphine or fentanyl. Derived from the poppy plant, evidence of human use of opioids for both medical and recreational use dates back more than 5000 years to ancient Sumer. The body naturally produces opioid substances, endorphin being the most well known. Activation of opioid receptors, either by endogenously produced opioids or exogenous opioids, induce a potent analgesia, dampening the sensation of pain. Opioid drugs are the current gold standard for pain relief. They also cause sedation and feelings of euphoria.
Heroin and morphine are frequently taken via intravenous injection, but many prescription opioids, particularly for long-term pain conditions, are consumed orally. Over the past 20 years, there has been a dramatic increase in the number of opioid-overdose-related deaths. The most recent spike in deaths is due to overdose on synthetic opioids such as the extremely potent painkiller fentanyl, which saw a 10-fold increase between 2013 and 2017. The so-called opioid epidemic kills an estimated 130 individuals from the United States each day.
Cocaine
Cocaine is a psychostimulant that is derived from the coca plant. The most common routes of administration are insufflation (powder cocaine), inhalation (crack cocaine), but it can also be solubilized and injected or taken via transbuccal and oral administration by chewing the leaves of the plant. Cocaine is considered to be a potent sympathomimetic, meaning the substance activates the sympathetic nervous system. Therefore, the physiology of a person on cocaine will be similar to an activated “fight-or-flight” response: elevated heart rate and blood pressure, dilated pupils, and increased respiration. Cocaine is a Schedule II substance. Although it has a very high addiction and harm potential, it has a handful of medicinal applications as well. For example, it is a potent local anesthetic and vasoconstrictor, so it is often used in surgery, especially in facial or nose surgeries.
Psychedelics
Psychedelics are the class of drugs formerly called hallucinogens. They can be either natural, such as psilocybin which is derived from mushrooms, or man-made, in the case of lysergic acid diethylamide (LSD). Psychedelics can cause a person to experience visual distortions, synesthesia, an altered sense of self (ego dissolution), or sometimes a sudden connection with nature or a higher power. Although psychedelics have been used for centuries in religious ceremonies, they have had a troubled history in the US. The adoption of LSD (acid) by the counterculture movement during the 1970’s, secret CIA funded research, and some loosely regulated research ethics in the clinical setting all led to notoriously negative press regarding the substance, tainted the general public opinion about this class of drugs. Since 2010, there has been a growing body of evidence supporting the notion that psychedelics can serve a therapeutic purpose, most notably in treating psychiatric conditions such as post traumatic stress disorder, terminal illness-related depression, and drug addiction.
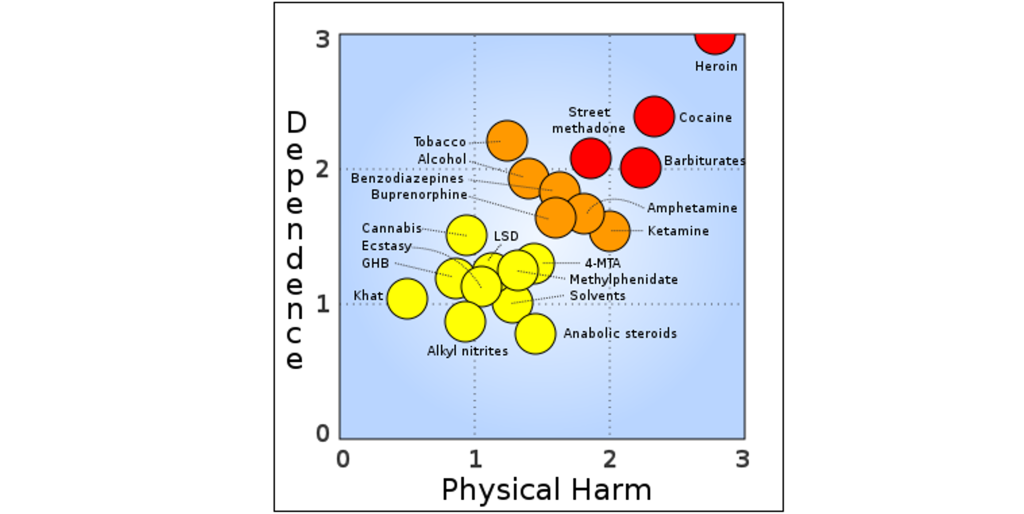
Comparing different drugs based on their potential for drug dependence and the amount of physical harm that they cause reveals that drugs such as heroin are classified as more dangerous.
Biology of Substance Use Disorder
Brain Structures Important in Substance Abuse Disorder
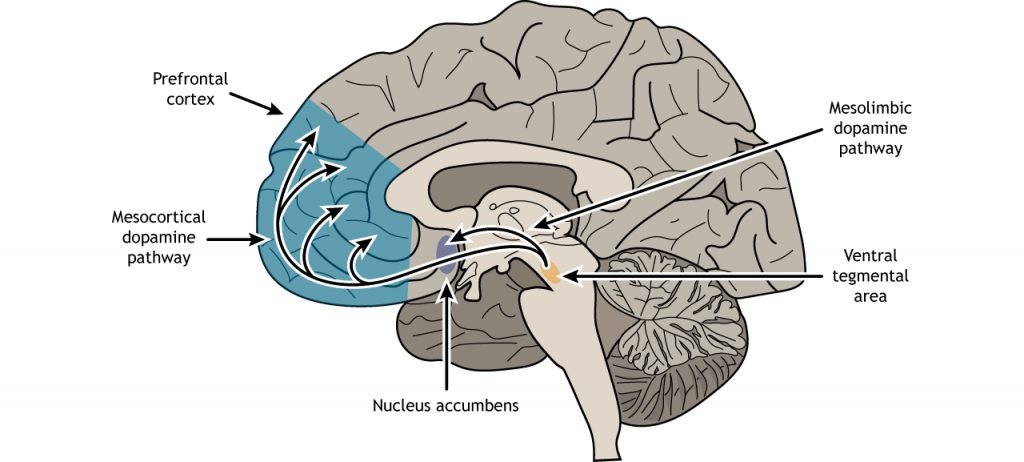
The mesolimbic dopamine pathway within the brain underlies reward (discussed in Chapter 49). As a reminder, our reward signaling neural circuitry starts with the ventral tegmental area (VTA). Located in the midbrain, the VTA contains neurons that synthesize the neurotransmitter dopamine (DA). These VTA DA neurons send their axonal projections predominantly into two main areas.
The mesolimbic pathway consists of dopamine producing neurons that release dopamine onto the cells in the nucleus accumbens (NAc), serving as the major pathway by which reward is mediated by the brain. A separate group of dopaminergic neurons in the VTA project to the prefrontal cortex in the mesocortical pathway. Drugs of abuse act on this pathway, causing drugs to cause heightened feelings of reward, making it more likely that individuals engage with these substances.
The nucleus accumbens can be subdivided into two portions called the nucleus accumbens shell and nucleus accumbens core, each with their own circuitry and functions. The nucleus accumbens shell functions in the “wanting” involved in drug addiction, as well as reward and reinforcement. The nucleus accumbens core, however, functions in the motor functions related to reward and reinforcement.
Plasticity
Plasticity in Dopamine Signaling
Using microdialysis, it is possible to measure the dopamine concentration in the NAc during performance of some behavioral tasks. In studies with rats, engaging in rewarding activities such as eating or sex results in increased release of dopamine in the NAc. Similarly we see that release of dopamine into the human NAc is enhanced when we engage in activities we enjoy: binge eating sugary stuff, having sex, even playing video games. Notably, many drugs of abuse such as cocaine or amphetamine can induce a similar overflow of dopamine release when an animal is exposed to the drug.
Many drugs of abuse cause a sensitized increased in dopamine release, meaning that there is an increase in dopamine release. Sensitization is a phenomenon in which there is an increased effect of the drug with chronic exposure. The increased dopamine release at the nucleus accumbens causes an increase in dopaminergic signaling, which can then lead to structural plasticity.
Structural Plasticity
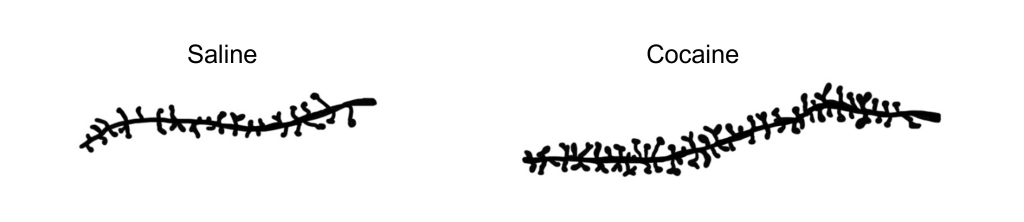
Repeated administrations of multiple drugs of abuse causes cellular plasticity within the nucleus accumbens and other structures within the reward pathway, by increasing dendritic spine density. Dendritic spines are small protrusions off the main dendritic shaft of neurons. They serve as the excitatory synaptic inputs for these cells, increasing excitability. Notably, though the increase in dendritic spine density is observed following administration of multiple drugs of abuse, it is not a universal structural change as opiates do not produce the same dendritic spine increase.
Actions of Drugs at the Synapse
Cocaine
Cocaine acts on a molecular level by functioning as a dopamine reuptake inhibitor, preventing the transporter protein from clearing the neurotransmitters such as dopamine out of the synapse. This leads to increased concentrations of dopamine in the nucleus accumbens and prefrontal cortex. This increased dopamine results in a greater likelihood that the postsynaptic receptors get activated.
Amphetamine
Amphetamine acts similarly to cocaine at the synapse, blocking the dopamine transporter and preventing reuptake into the presynaptic cell. Amphetamine can also mimic dopamine at the dopaminergic synapses, binding to dopaminergic receptors.
Opioids
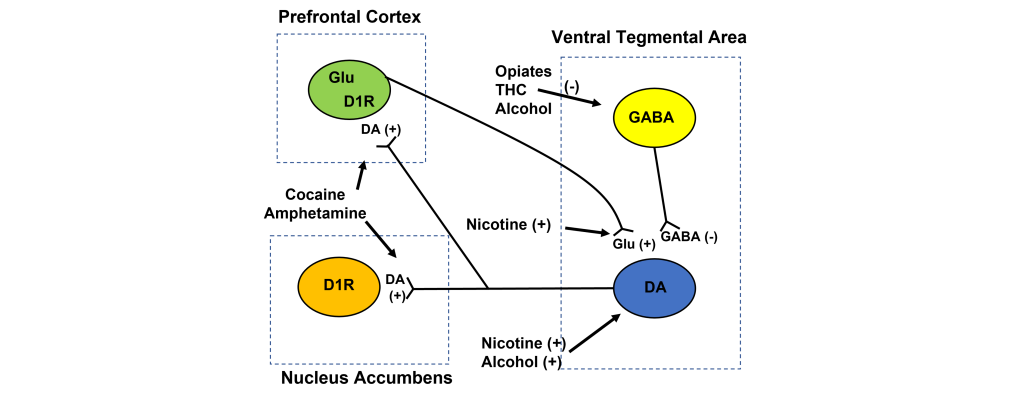
Opioids being to GABAergic neurons, causing them to hyperpolarize and suppress release of GABA onto dopaminergic VTA neurons, disinhibiting the VTA neurons and increasing dopamine release onto downstream targets.
Cannabinoids
Although the cannabis plant contains several chemical substances, the main psychoactive ingredient is delta-9-tetrohydrocannabinol, or THC for short. THC, once it enters the bloodstream, is capable of activating receptors that our body uses endogenously, called the cannabinoid receptors (CB receptors). THC inhibits activity of GABAergic neurons that synapse on the dopaminergic VTA neurons, disinhibiting the VTA neurons and increasing dopaminergic signaling.
Nicotine
Pharmacologically, nicotine has specificity as an agonist at nicotinic acetylcholine receptors (nAChRs), excitatory ionotropic receptors that are expressed widely across the body. When nicotine binds to VTA neurons,it activates the cells and causes an increase in dopamine release. Nicotine can also increase glutamatergic activation originating from the prefrontal cortex onto VTA neurons. Collectively, this acts to increase activity of VTA neurons and increase release of dopamine at downstream targets.
Alcohol
Ethanol is a tiny molecule with properties similar to water, meaning that ethanol can diffuse easily through cell membranes. Whereas other chemical substances often have highly specific molecular or protein targets, ethanol has several. Ethanol activates dopamine neurons within the ventral tegmental area, causing an increase in dopamine release at the nucleus accumbens. Further, alcohol acts to inhibit GABAergic neurons within the VTA, disinhibiting the dopamine neurons and increasing their signaling.
Tolerance and Sensitization
Tolerance
Pharmacologically speaking, tolerance can be defined as a decrease in the action of a drug due to repeat exposure. This phenomenon happens as a result of homeostatic adaptations that the body undergoes when it has been exposed to a substance for a prolonged period of time. In a person who is tolerant, they must take progressively higher doses of the drug to experience a desired effect. For a drug naive person, someone with no experience with the drug, a low dose of drug may have a strong effect. However, for a person who has become tolerant to the effects of the drug, that same low dose will produce a small drug effect.
There are different forms of tolerance that a person can experience. In metabolic tolerance, there is a decrease in the amount of the drug that gets to the site of action. The body becomes more efficient at eliminating the substance. Since exogenous substances usually get degraded by enzymatic reactions, an increase in the activity or number of enzymes will decrease the amount of the substance that is capable of acting.
The most common example of metabolic tolerance is seen in frequent alcohol use. The main psychoactive substance found in alcoholic beverages like beer, wine, or liquor is ethanol. Our liver, which filters circulating blood, contains enzymes which break down chemicals in the blood. Specifically, the standard degradation process of ethanol uses two enzymes. The first of which, called alcohol dehydrogenase, oxidizes molecules of ethanol into the toxic byproduct acetaldehyde. The second step uses the enzyme acetaldehyde dehydrogenase to convert the acetaldehyde into acetic acid, a generally harmless compound (the same chemical structure as vinegar) that is used by the body in a biochemical reaction that drives the citric acid cycle. Because most alcohol is taken via oral consumption, ethanol is subject to first-pass metabolism before reaching systemic circulation.
However, after prolonged exposure to alcohol, the body undergoes homeostatic compensatory changes. The two liver enzymes responsible for degradation of ethanol increase in either function or amount. When these metabolic enzymes become upregulated, the circulating ethanol in the bloodstream becomes broken down more rapidly and more efficiently, resulting in a decrease in the amount of ethanol that reaches general circulation, and consequently, the brain. This explains why people who have never drank alcohol (low amounts/function of enzymes) may experience a stronger drug effect compared to someone who drinks regularly. It also accounts for why there is some genetic variation between a person’s sensitivity to alcohol’s intoxicating effect, as enzyme efficiency is partially encoded by genetics.
Another way by which tolerance can manifest itself is through changes at the level of the molecular components of cells. This type of tolerance is called cellular tolerance. This tolerance leads to a decreased sensitivity to the substance. Cellular tolerance can be characterized by a decrease in receptor expression after chronic exposure to an agonist. When the opioid etorphine is present in the body, it activates the opioid receptors. Frequent exposure to etorphine causes a molecular change in the receptors, which leads to internalization, the process by which cell surface-expressed receptors become taken into the cell. Since etorphine is only able to activate receptors on the surface, these internalized receptors diminish the strength of the etorphine signal, which manifests as tolerance. By downregulating the number of receptors that are expressed on the surface, the cell reacts to the environment by becoming less responsive in the face of drug.
Sometimes, the body physiologically prepares for the drug effect before the drug is even present. The way it does this is to initiate an opposite somatic effect from what the drug is expected to do. This “reverse” effect is likely a protective mechanism to minimize the drug effect, and these anticipatory bodily changes can be precipitated by drug-associated cues. For example, heroin causes analgesia. Cues that predict administration of the drug, such as preparation for an intravenous injection or being in a physical environment where drug is frequently administered, can cause the reverse physiological effect, hyperalgesia. Because of this, a person may need to take more drug to overcome the anticipatory changes. This unconscious form of learning leads to a form of tolerance that is dependent on Pavolvian cues; this is called conditional tolerance. If not accounted for, conditioned tolerance can have potentially lethal side effects. A clinical description (Siegel, 2001) of a patient with pancreatic cancer describes one such “failure” of tolerance. Bedridden and suffering from tremendous pain, a man was regularly given morphine in his bedroom, dark and filled with humming apparatus for his medical care. As expected, he developed a tolerance towards the morphine, requiring higher and higher doses in order to inhibit pain. One day, he went into the brightly lit living room to receive his normal dose of painkiller. Soon after, he died from opioid overdose.
Sensitization
Sensitization is a phenomenon related to tolerance, but the polar opposite: instead of a drug effect being lessened after chronic exposure, a sensitized person experiences an increase in drug effect. Nicotine as well as many psychostimulants such as cocaine or amphetamine can produce psychomotor sensitization after repeated dosings. Psychomotor sensitization can be measured through crossovers (how often the animal runs across the midline of the cage). Animals displaying sensitization will show significantly more crossovers compared to non-sensitized animals. This sensitization can be long-lasting, remaining for up to one year following the last dose of drug.
Using Animal Models to Study Abused Substances
“Why do some people transition from user to addict?” Many people are able to use the most addictive substances such as cocaine or heroin casually without ever becoming an addict. For these people, their drug use pattern can remain recreational, even though they may use the substance frequently and report a great sense of satisfaction when they use the drug. On the other hand, there are some people who have a very high propensity to quickly becoming a pathological addict. One of the big challenges in drug abuse research is to understand the differences between these two populations. What factors, either environmental or genetic, are protective and prevent the transition from casual drug user to compulsive drug addict? And what are some ways we can use this knowledge to help addicts find ways to break their pattern of harmful compulsive drug seeking and drug use? One possible way to get at the answer is to create animal models of drug dependence and try to determine the nature of the underlying biological changes that contribute to the addiction-like pattern. Do some cellular circuits change permanently? Are certain genes or proteins upregulated or downregulated? Can pharmacological or behavioral interventions change drug-taking or drug-seeking behavior?
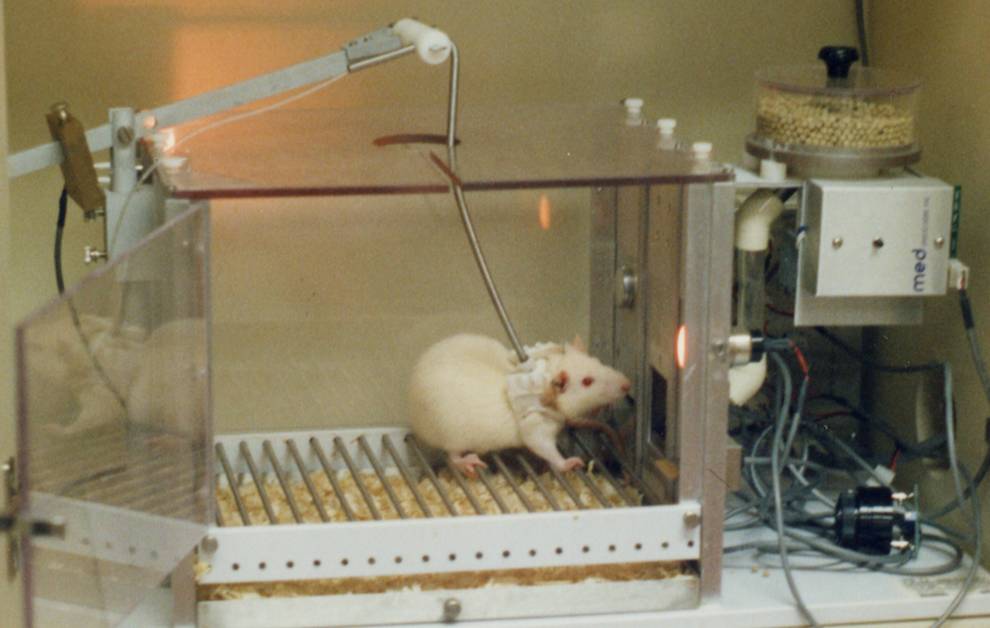
Self-Administration
One of the most instructive non-human animal models of drug use disorder is called self-administration. In a self-administration experiment, the subject (usually a monkey, rat, or mouse) gets a surgical implantation of an indwelling intravenous tube that is connected to a pump. Then, the subject is put into an operant conditioning chamber. When they press the lever or poke their nose into a hole, the pump triggers, resulting in an infusion of drug directly into the bloodstream. This experimental paradigm closely mimics human drug seeking behavior. For example, rats and mice will very quickly learn to press on the levers for intravenous infusions of cocaine and morphine. Many of them will give themselves drugs even despite severe adverse consequences, such as enduring foot shock—arguably similar to human behavioral patterns where addicts may do all kinds of behaviors for access to drugs. Monkeys, if given the option to self administer for cocaine, must be restricted in the amount of drug they receive: if given unrestricted access, they give themselves so much cocaine that they have seizures and die.
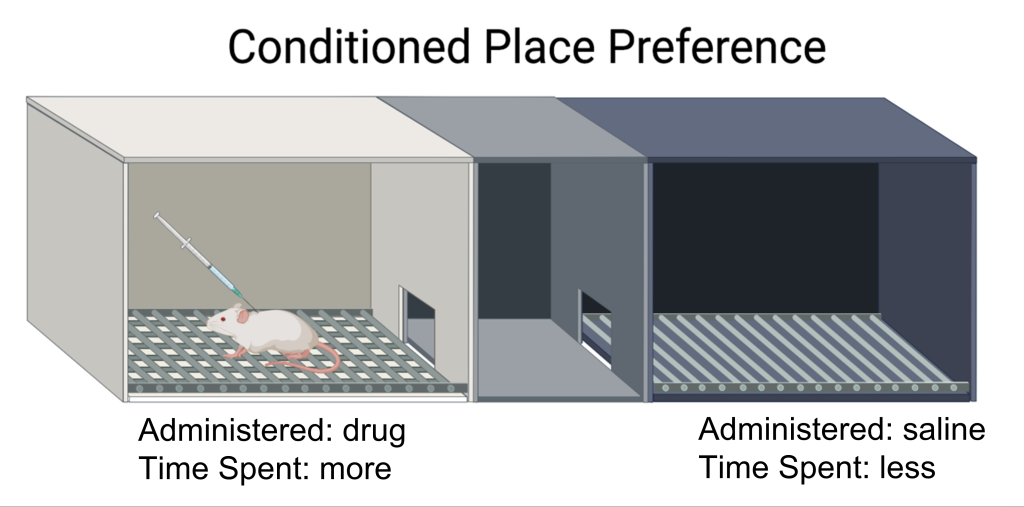
Conditioned Place Preference
A second experimental test created to study drug abuse is called conditioned place preference (CPP) (also discussed in Chapter 50). A CPP test works on the principle that animals learn to associate certain environments with positive feelings, and will prefer to spend significantly more time in those environments. To conduct CPP, a three-room testing chamber is used. This experimental chamber has two large rooms, each with characteristics that are unique to that room. For example, one room may have mesh flooring with dark-colored walls, while the other room may have woodchip flooring with light-colored walls. The two rooms are connected by a smaller, neutral room, and the rooms can be isolated from another by means of a dividing door. To conduct CPP, an animal will be given the drug of interest, then placed into one of the two rooms, where they are free to explore the room, but cannot leave. As a control, at a different time, they will be injected with an innocuous solution and placed into the other room. On test day, the animal will be put into the neutral middle room, and given the opportunity to move freely between the two chambers. If the animal developed positive associations with the room where they experienced the drug effect, then they will choose to spend significantly more time in that room. On the other hand, if they experienced negatived conditioned place feelings associated with that room, they will avoid being in the room. Whereas self-administration assesses “drug seeking”, CPP measures “drug liking”.
Hypotheses to Explain Substance Abuse Disorder
Below are three major biology-driven hypotheses that have been proposed to explain drug addiction. It’s important to note that none of them tell the complete story—otherwise drug addiction will have already been cured! Also, these theories are not mutually exclusive from one another. A likely answer to curing addiction probably incorporates some combination of these approaches in addition to societal policy changes.
Hedonia Hypothesis
What drives addicts to behave in the way they do? One of the earlier theories put forward to explain addiction is the hedonia hypothesis proposed in the late 1970s by Roy Wise. The hedonia hypothesis hinges on the assumption that dopamine is the “pleasure neurotransmitter”, and that any substance or behavior that increases dopamine will be desirable. The theory is supported by some behavioral data. For example, using microdialysis, it was found that dopamine release by the mesolimbic pathway increases in the presence of many drugs of abuse. Additionally, administration of dopamine antagonists are able to block some drug taking behavior. This dopamine-centric approach to drug use disorder was so influential that pharmaceutical companies, while developing novel antidepressants, quickly dismissed drugs that increased dopamine out of fear of the risk of addiction potential.
Despite the attractiveness of the straightforward “pleasure neurotransmitter” model, the dopamine hypothesis does not give us the whole picture. For one, dopamine release at the mesolimbic pathway is only notable for psychostimulant drugs, such as cocaine and methamphetamine. But there are plenty of stimulants that still produce the significant overflow of dopamine without causing any rewarding sensation. Furthermore, if dopamine is the signal that mediates the positive hedonic feelings, one might predict that by blocking dopamine receptors chronically, you can also prevent long-term cocaine addiction, but this therapeutic strategy isn’t very useful. Many of the most popular misconceptions about dopamine that you frequently see in the media take this early hypothesis as the truth. It even was featured as the cover of a 1997 Time magazine. That same year in an interview with the original proponent of the hedonia hypothesis published in Science, Roy Wise agreed with recent results that his model was incomplete.
Incentive Sensitization Model
A more recent theory to explain drug addiction is a model developed by researchers Terry Robinson and Kent Berridge from the University of Michigan. Under their model of drug use, initially a person takes a drug because they like the positive, euphoria-producing side effects of the substance. But after chronic exposure to the substance, the person becomes fixated on obtaining the drug rather than how the drug makes them feel. At this point, they continue to use the drug even though they no longer enjoy the drug to the same degree that they once did. Instead of “liking” the drug, the addict fixates on “wanting” the drug. The incentive sensitization model suggests that the drug-exposed brain develops an increased sensitivity to drugs, but also more importantly, drug related cues.
Pavlovian learning takes place when an addict takes a drug. Each drug has an associated set of cues, and reexposure to those cues can trigger relapse. Over repeated pairings, those cues trigger a progressively stronger response. Their model accounts for why it is difficult to remain abstinent from an addictive drug for long durations of time. Despite a decrease in drug seeking behaviors, many addicts eventually relapse, or return to the previous destructive pattern of drug use. One phenomenon that makes staying drug free difficult is the observation that prolonged abstinence can increase the intensity of drug cravings. This is called incubation of craving, and is seen with several different classes of drugs, notably, nicotine.
Brain Disease Model of Addiction
Much of our current understanding of addiction is based on the principles that repeated drug use leads to biological changes in the brain that resemble aberrant learning. This model for drug addiction is called the Brain Disease Model of Addiction. Genetics has a strong influence on the likelihood that someone develops a disease, and addiction is no different. Inherent risk-taking behaviors, magnitude of a drug effect, and risk of relapse are all modified by genetics. One of the major implications of this model is that compulsive drug use and seeking is not a choice that a person makes. Addicts are not the way they are because of some poor moral guidance or a weakness of willpower. Addicts compulsively seek drug because of some underlying circuitry of their brain that makes cessation difficult.
One substantial accomplishment of this model is that public policy has adjusted to increase access to mental health resources for addicts to help cover the financial challenges of recovery programs (Mental Health Parity and Addiction Equity Act of 2008), and to improve the outcomes of nonviolent drug offenders as they reintegrate with society outside of prisons. This model is not without fault, however. The major criticism of this framework to explain compulsive drug use is that most people stop their addictive use patterns by themselves spontaneously without any treatment. Another harm of the Brain Disease Model of Addiction is that it puts heavy emphasis on biochemical therapies rather than on a public policy approach to drug addiction treatment. Lastly, this model has not produced a successful therapeutic strategy to help with addiction.
Attributions
Portions of this chapter were remixed and revised from the following sources:
- Open Neuroscience Initiative by Austin Lim. The original work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
Key Takeaways
- The DSM-5 is used for diagnosing substance abuse disorder.
- Drugs of abuse act on the mesolimbic dopamine pathway to make drugs rewarding.
- Increased dopamine signaling can lead to structural plasticity, such as increased dendritic spine density.
- Drugs of abuse have different sites of action within the mesolimbic dopamine pathway to ultimately cause an increase in dopamine signaling.
- Drug tolerance causes a decrease in drug action with repeated use, whereas drug sensitization causes an increase in drug action with repeated use.
- Animal models of self-administration and conditioned place preference are used to better understand mechanisms of drug action.
- There is not one complete hypothesis of drug addiction.
Media Attributions
- DSM5 © Yoshikia2001 adapted by Valerie Hedges is licensed under a CC BY-SA (Attribution ShareAlike) license
- Graph comparing dependence and physical harm © Apartmento2 adapted by Valerie Hedges is licensed under a Public Domain license
- Dendritic spines © Valerie Hedges is licensed under a CC BY-NC-SA (Attribution NonCommercial ShareAlike) license
- Drug action © Valerie Hedges is licensed under a CC BY-NC-SA (Attribution NonCommercial ShareAlike) license
- Self Administration © Jinrikisha Amufabalo adapted by Valerie Hedges is licensed under a Public Domain license
- CPP © NeuroFall2021 adapted by Valerie Hedges is licensed under a CC BY-SA (Attribution ShareAlike) license
chemical substances that come from outside the body
breathing in
administered through the cheek
administered through the skin
decreases pain
blowing something into a body cavity
dopamine producing neurons that start in the ventral tegmental area and project to the nucleus accumbens
decrease in the action of a drug due to repeated exposure
increased effect of a drug after repeated administration
Behavioral paradigm that measures reward associated with an envirorment

{kind=link}
.svg){kind=link}
{kind=link}
{kind=link}